
Here’s what myofunctional therapy is and how it can help with sleep apnea, snoring, jaw pain, tongue ties, mouth breathing, UARS, TMD, ADHD symptoms, bedwetting, and more! In my interview with Melissa Johnston, a myofunctional therapist with Faceology, we discuss why tongue posture is the foundation of airway health, how the three pillars of structure, function, and habits explain so many of our struggles, and what you can do about it for yourself and your children… plus my own story of going from terrible sleep to sleeping great again!
Table of Contents

Waking up exhausted… jaw pain… snoring… brain fog… getting up multiple times a night to use the bathroom… not being able to breathe through your nose. Sound familiar?
These are signs of orofacial myofunctional dysfunction, and they affect far more people than you’d think.
I know because I was one of them. My sleep had gotten so bad that I was ready to get on a CPAP machine. I was desperate. That’s when I found myofunctional therapy and started working with Melissa Johnston.
After several months of working together, I’m happy to say I’m sleeping great now. But here’s the thing… now that I’ve seen what these dysfunctions look like, I can’t unsee them. I see the signs in children, in adults, everywhere. And I realized that Melissa’s expertise could help so many people, not just those of us who are already struggling, but the younger generation, too. If we can catch these issues early, we might save our children and grandchildren from the pain and sleeplessness that so many of us deal with later in life.
Melissa Johnston is a dental hygienist of 20 years and a certified myofunctional therapist who works with Faceology. She sees patients ages five to eighty, via telehealth in the U.S. and internationally. Her journey into myofunctional therapy began when her own daughter was struggling with chronic sinus infections, obstructive sleep apnea symptoms, and multiple surgeries… and conventional approaches weren’t getting to the root of the problem.
In this interview, we’re going to look at how myofunctional therapy addresses the root causes of sleep issues, breathing problems, jaw pain, and so much more. If you or someone you know struggles with snoring, sleep apnea, TMJ pain, mouth breathing, or if you have children who are picky eaters, bedwetters, or showing ADHD-like symptoms… please listen to, watch, or read this interview with Melissa Johnston from Faceology to learn how myofunctional therapy can help.
In this article:
- why tongue posture is the foundation of sleep, breathing, and facial development
- what myofunctional therapy is and the three pillars it addresses (structure, function, and habits)
- what tongue ties really are and how they’re graded
- how the fascia system connects your tongue to the rest of your body
- why women in perimenopause and menopause are especially affected
- red flags to watch for in children (and why it matters for ADHD, bedwetting, and picky eating)
- how Melissa approaches treatment and what to expect
- and much more!
Please set aside distractions and watch or listen to the video below. Or, if you prefer to read, the complete transcript plus my summary notes are below!
Wardee: Hey everyone. Welcome. I'm Wardee with Traditional Cooking School, home of the Eat God's Way cooking program, and I'm joined today by Melissa Johnston. Hi, Melissa.
Melissa: Hi. Thanks for having me.
Wardee: It's so great to have you. Let me just give you a quick intro to Melissa, but she's going to share more about her story.
Melissa and I have been working together for several months now. I came to her actually for myofunctional therapy because I found out I had a tongue tie, but what was really happening was my sleep was terrible. And when something gets so bad, you're like, I have got to fix this. So after working with Melissa, I'm happy to say I'm sleeping great now.
But the thing is... and maybe this is the funny thing... now that I've seen what the dysfunctions I had can do, I can't unsee it. So I see it everywhere. I see it in children, adults. Oh, you just can't unsee these things. So what I did was I asked, Melissa, will you please let me interview you, because I feel that she can help so many people.
She can help those of us that are struggling, but also hopefully the younger generation, because if we could save them some of the pain that we get to as we get older and we can't sleep or have trouble breathing or whatnot, I just think that's so worth doing. So Melissa, thank you for agreeing to come and share your expertise with us.
I know we're going to learn a lot and it's going to be so encouraging. Thank you so much. If you would just share... let's start with the tongue and the tongue position. Why and how does that play such an important role in our sleep, our breathing, and our quality of life?
Melissa: That's a perfect place to start. So I don't know if your listeners know really where their tongues should live. And when I say that, that's at rest. So if you're not speaking, if you're not eating or chewing, when you are at rest, I would prefer your tongue to be up in the roof of your mouth, lightly suctioned, filling into your palate.
And people go, well, why does that matter? It matters because... let's go from the beginning. Whenever you are born and whenever you are forming, we need your tongue up there because it starts how you functionally grow and form. When your tongue's in the correct position, it's acting as the scaffolding of the course. The upper palate... we want your palate to be a nice U-round shape, but it's also acting as the floor of the sinuses.
So instead of growing into, let's say, a narrow phenotype... which, guess what? That's what I am. I'm the very thin... well, it used to be thinner... face, the thin nose. I don't know if you can tell that the little deviated septum and hump in the nose. I was a thumb sucker. I'm going to jump around a little bit, but I hope what I say pieces things back together. But muscle will beat out bone in the long run, and that's everywhere in your body. Your tongue has 600 grams of pressure alone, and so that's a really large muscle in your body.
It does a lot of things. Also, your cheeks and lips... that's a part of what we work on too. But let's say your tongue is low, how mine was. My body was craving something to be up. I compensated, which is a word we'll talk about too, and wanted my thumb up there. The body's going to get what it needs, whether it's a good habit or a bad habit.
My body was craving something. I became a thumb sucker, so I formed into a very specific phenotype, which... I have chronic sinus issues. I didn't have the point of needing tubes. I know a lot of children now we see that, or needing tubes placed in their ears due to Eustachian issues. But I was pretty much a poster child of needing myofunctional therapy, but my mother didn't know what that was. I didn't even know what that was until a few years ago.
But with the tongue being up, let me get back to that. That's helping us form in more of a pattern that in the long run, our sinuses are going to be more open. We're not going to end up with a deviated septum. Our turbinates are going to be able to function. When the tongue is also up and the lips are sealed, of course, daytime, you're able to breathe, but at nighttime, that's really supportive of your airway when the tongue is up, the lips are sealed, our soft palate is supported, and so therefore we have more room for our airway to have oxygenation pass through.
I'm going to jump back up to the nose at that point. So as we breathe in through our nose, our body creates something called nitric oxide. It's something that God put in us. That's a wonderful kind of chemical that helps to support... it brings more oxygenation in. It's a vasodilator. It keeps the blood moving around a little bit better. And a really cool effect of it... it's an antiviral and antibacterial once it enters the lungs. So think about all the stuff that we have in the air these days, and I won't even get on that. I can totally go off left field from what we're breathing in, but it's a way to filter and get more of a better saturation of oxygenation into our lungs as we have our tongue up. And that's how we should be fully supported.
So day and nighttime, tongue in the right position, lips being sealed, nasal breathing. That's what we're aiming to do whenever you work with a myofunctional therapist.
Wardee: Amazing. Thank you. And it makes you think God's design is so perfect. His system supports the best health possible.
Melissa: 100%. I grew up in a very medical background, and I know a lot of times people want to say there's a separation of this and that, and I don't feel that way at all. I feel like if you can learn how the body functions, you have to admit that there was a perfect designer because that just... that doesn't happen by accident. Everything is so integrated in how it works together. It's amazing. And yeah, we're a very integrated system. He had a lot of insight whenever he was putting those things in place.
Wardee: God is good. Okay. And you just brought up the idea of myofunctional therapy, and you have told us about the proper functioning of the tongue, posture, compensations we do. So lead us into... when we do have dysfunctions, either learned or actual physical defects... what is myofunctional therapy? How can it help us?
Melissa: So myofunctional therapy... it's just a big word for PT, physical therapy of the head, neck. We're working on the face, we're working on the tongue, we're working on the lips, the throat. Of course, that all goes back into the airway world. But what we're doing, as far as some basic foundational goals... I listed a little bit. We're working on correct tongue posture, we're working on lip seal. When our tongues and lips are working together, of course, we're getting the best benefit for our nasal breathing. That's one of our goals... nasal breathing. And I actually work on chewing and swallowing.
I like to go back to thinking of our bodies as in three pillars. We have our structure and form, we have our function, and then we have habits. And just to even go back to me as a phenotype and how I grew... since I had a low tongue function, that caused my form to turn into what it's doing now. And I developed a thumb-sucking habit because my body was craving something. And we rotate in and out of those columns and pillars. So if we can figure out, let's say, this is a negative habit, I can go in with myofunctional therapy and the exercises that we're working on to correct habits.
We have different things that we teach with awareness. We have different modalities that we use with different appliances... for instance, pacifiers and thumb sucking, to that nature. I have different... I can show you one right here. This is called a Myo Munchee. This is an appliance that I use to get children over that hump, or give them something. Let's say we're going to take away a bad habit and put in a better habit over it. So we have corrective things that we can put in place, and different awareness and tactile cues that we use to eliminate a habit so we can start working on a better function.
Because also with myofunctional therapy, I'm teaching the patients a certain level of awareness with their body. Compensations was a word that I used, and that you know about. But compensations is basically... the body needs to do something and it's going to do what it has to do to obtain it, and it can be negative. So a lot of my patients, when they come, if they've been dealing with this for a while, they can have forward head posture. Forward head posture over time can cause different issues going down, because we're a system. It can turn into lots of neck strains. Some of the compensations that we work with... people are using more of these accessory muscles. It can turn into jaw instability. So we have jaw lateralization and protrusion. There's just different ways the muscles are going to try to help, even though it's not a good pattern that they're helping with.
So we help the patient identify when those muscles are kicking in and engaging, get them to correct those habits, and also build strength and awareness to the muscles that we do want to integrate and work correctly.
Wardee: Wonderful. Can you name those three pillars again?
Melissa: Yeah. So we're working with structure and form, you have your function, and then you have your habits.
Wardee: Structure, form, function, habits. Could you give us an example? I did not prepare you with this question.
Melissa: No, you're fine.
Wardee: But it just made me think... you gave yourself as a great example. Let's do another example of a tongue tie. What would you see with a tongue tie with those three pillars? What would happen?
Melissa: So tongue ties... whenever we're saying tongue tie... and a lot of people too, I try to express this way... people think of tongue ties as they're not able to just stick their tongue out. It's not that true definition. So as a myofunctional therapist... and I always have patients, especially whenever you have mothers that just had babies, I have babies... I want people to work with IBCLCs. They're specialized lactations. A little bit more integrated than just a normal lactation specialist. They have a lens, just like I have a lens now for identifying a restricted tongue.
So it's not how the tongue looks, it's how the tongue functions. That's a lot of how we're doing things. So I don't want to discredit people, but for instance, I've been a hygienist for 20 years. I've worked with two exceptional dentists. I'm not going to say they're the greatest at identifying that, because they don't have that specific lens like I do now. And it's more of how the tongue functions. I have patients do different things whenever I test them, and I have them do some certain swallow activities. I have them do some different ways that they're reaching their tongue and moving things. I have them pronounce different sounds. There's ways to identify it, and it doesn't have to be so prominent.
So we have it graded. We have grade 1, 2, 3, and 4. Grade one would be... not a tongue tie. It can even just be low muscle tone. So whenever we started talking, you said you were diagnosed with a tongue tie, but I'm going to say everybody has a frenulum. So when I say frenulum... yeah, the tissue underneath the tongue... that is how restricted that frenulum is. You definitely had some restriction, but it wasn't to the degree that you needed a release. Yours ended up being more low muscle tone that we were able to work on and obtain where we needed to get those goals. So in the end, it wasn't a full restrictive tongue.
So coming back to a tongue tie... a true definite tongue tie... this is where, let's say, compensation-wise, the person expresses as, oh, they can talk and they can do different things and they move. But the back or middle of the tongue is never able to fully get into the palate. The tip is up there, but the back's never fully able to get up there. If you can believe this or not, I've had three different SLPs... so an SLP is a speech language pathologist. Two of them were tongue tied. One of them was low muscle tone. So their job is to teach people how to speak and how to eat and how to function, and both of them actually had restrictions. So they were just as shocked as I was. I was like, wow.
But in the long run, that's what we do. We start off and we try to teach the muscle tone, and we try to get things in balance to see if this restriction's going to cause issues and if we need to have a release. So if the tongue is truly tied, it's not able, like I said, to fully get up into the palate. So the form will end up being more narrow. I'm not saying that they end up being a pacifier user or a thumb sucker, but typically their form will end up being more narrow because the tongue was never that structural support like I said, needed to be.
Then they can develop habits. So when the tongue is low, a lot of times that muscle tone becomes low, they end up usually having some type of mixed breathing. So they might do a little bit of nasal breathing, a little bit of mouth breathing, but they tend to end up with more mouth breathing, especially at night. And so then you end up with other habits and different things, and the body starts going through that snowball effect of... it turns into not just airway issues, but overall symptoms... the body starts to have inflammation and different things.
So yes, the structure's messed up because of the function of the tongue, because the tongue was tied, and then you develop other habits. Like I said, it goes in and out of those pillars just with what's going on.
Wardee: You probably see similarities, but you probably see people who... there's just a uniqueness in how the form gets expressed down the line and then where they end up with the dysfunctions and the pain.
Melissa: Absolutely. Again, the body's a system, and I try to think of our bodies as domes. We'll talk a little bit about this, I'm sure, as we keep talking. But there's a lot of similarities between our pelvic floor, our pelvis, and our temporomandibular joint... how it functions and how it rotates. So you can have issues down in the pelvic floor, and it can actually come up and express here as well.
I know I'm jumping around a lot. We are just one part of a bigger system. Whenever you work with myofunctional therapy, you're probably going to end up working with an orthodontist, an ENT, a dentist, a body worker. So body work can be pelvic floor therapist, it can be craniosacral therapist. But our body is so integrated with a fascial system. So fascia is a key term people are talking about a lot lately, which I love, because there's this new understanding that's coming, that there's a whole nother layer in there that people didn't realize is happening.
So you have a frontline fascia. It goes from the tip of your tongue to the tip of your toes. And what's really neat about that, especially in some of my younger kids... my older patients sometimes feel this too... but let's say they have a tongue tie and they need a release. Whenever that doctor goes in to do that treatment with a laser, once that fascia is released in that area, I've had patients come back and tell me that their chest opened up, that their shoulders dropped. I had one patient tell me that they didn't even realize how tight their feet were constantly, and they felt like they relaxed. So there's incredible entangling that's happening with that whole system.
So going back to the domes, you have our upper palate, our esophagus, our diaphragm, our pelvic floor, all the way to the arches of our feet. So if something gets a little out of whack in any of those areas, it can ascend and descend through the body. And a lot of times, if it's happening here, you might feel it in other areas as well.
Wardee: Oh, fascinating. Thank you for sharing that. I'm putting it in perspective now. I want to turn a little bit so you can share your story, because you didn't start out as a myofunctional therapist. You started out as a hygienist. So I'm really curious how that all happened.
Melissa: I give the credit to, of course, the Lord, putting this on my heart and going, this is not right. But my daughter was my big highlighter. Of course, I've realized now that I had all these issues, but she is the one that helped me to deep dive and realize this was something of a modality that I needed to learn, I needed to be able to integrate, help other patients with.
But in 2018, she was five at the time. This was after she had tubes placed twice. This was after a sinuplasty and adenoids removed. I fought with the ENT... he wanted to keep her tonsils, and... I'm okay with it now. At the time I was furious. I'm like, why are we doing all the surgery? We're not taking these tonsils out. She was my obstructive sleep apnea kid to a T. But I live in South Georgia. I don't know if your listeners can tell by my accent... but we don't have a lot of airway knowledgeable practitioners in my area. So I was running into a lot of just brick walls when it comes to trying to figure out what's going on.
The ENT, of course, did these things, and that was very helpful, but she kept coming back. It wasn't that she was getting sinus infections anymore, but she kept coming back with these big snoring habits. And it wasn't constant, but it was... again, thinking of those pillars... she was not tongue tied, but I don't know if she started off when that allergy early, she started having these chronic sinus infections. Let's think about it. If you have chronic sinus infections, your nose stays stuffy. Therefore, what's your body going to do? You're going to start breathing through your mouth. When you breathe through your mouth, your tongue's going to drop. Therefore that air is going to keep passing through there. You're not going to get your nitric oxide. So your nitric oxide... not just all the cool things that it's doing inside your body... you can get kids that are having enlarged tonsils. If you can catch it in time and get them to lip seal and nasal breathe, that nitric oxide will actually take that tissue and shrink it back down and heal that tissue in the back.
So I learned about myofunctional therapy and I went, oh, this is it. This is what I've got to do. And things happened. My husband got a different position within his job, which got him really busy, and my child got really involved in different sports, and it got put on a pin. Like, it was there. I knew I needed to do something with it. 2019 happened, 2020, woo-hoo, COVID happened. And of course, I got deemed as a non-essential person, which blew my mind. Because I've been in the medical field for 15 years at that point. How in the world are you telling me I can't come to work?
So that slowed my body down a little bit to go, this is still happening in the background. Like, I've got to do something about it. I talked to some different people, and the airway world is getting bigger, but it's still pretty small, and there's some pretty large entities in it. I was able to speak to Sarah Hornsby and Melissa Mogno, and they said, if you want to do this, this is some of the courses I would recommend, and whatnot.
I was about to do it. And if I talk about it too much, I might start crying. At that time too, my boss that I worked with for 15 years unexpectedly got diagnosed with cancer and passed away within two weeks' time of a diagnosis. I'm not going to cry... he's in a much better place. But with that, that kind of took my sails out too. Every time I get amped up for it, something happens. This big corporate entity came in, and I learned really quick that I'm not a corporate employee. My husband, with the position he was in, he said, come home. Come home and grieve and take the time you need to do what you need to. And the Lord helped to really support me through that time, and gave me, again, the like... you've got to do this.
It finally worked out, because honestly, even if I wanted to integrate that into that practice that I had been working with for so long, my dentist was 70 years old. He was wonderful, but I don't know how open-minded he would have been to let me just full-fledged jump into this.
So it took some time. It took some doors closing and some windows opening. But I finally jumped in. I finally took classes with my mentor. I also realized, again, in South Georgia, I don't have a lot of support in this area. So it was starting to weigh on my heart, like, I have this new love and this new thing that I want to do and I want to incorporate and I want to teach people. And I had this big... it was nothing but divine intervention... I had this big weighing on my heart to reach out to Sarah, because she had just been working with Faceology. That's who I work with. But she has a different program after you exit... I'm still... sorry. My mentor, where you can go into and be mentored even more. They've got some different things in between. But Faceology is where, if you are a therapist and you want to work for her, she has a few spots that open up from time to time.
And I reached out to Sarah and I said, look, I know this is a long shot, but do you need somebody in little bitty South Georgia that could be available? And she said, I do, because I don't just work with people in the US, I work with people internationally. So my time zone being in the Eastern time zone actually helps a lot of patients over in Europe, because they're five and six hours ahead. So I work with a lot of people across the pond now. I think the furthest patient I've worked with was... goodness gracious... she was 17 hours ahead. I can't even think about now. I've worked with people in so many different time zones and whatnot.
But yes, it's been such a blessing because, even though I didn't think I was ever going to get it started here... which it's taken roots, I've got some doctors that are wanting to learn things now... but I've been able, since the word go, to incorporate it and get running and helping patients along the way. I know that was a lot, but yeah, that's how I landed here.
Wardee: I love it. What a great story. I love hearing how people get from point A to point B to point Z, and it's a winding trail, but God is so good. He doesn't let us let go of things. Actually, he does let us let go of things... but he's so good to keep us going when we're on the right path. That's beautiful. Thank you. Thank you for sharing all that and how great that in little South Georgia, you have local practitioners who are opening up.
Melissa: It's slowly working. And that's true even in other areas. I always try to tell my patients, you might have to travel to find the right person, because it's such a small criteria that people get and develop and learn that lens for. And I have very high standards when it comes to, especially if I'm going to have a patient have a tongue tie release. I'm not just going to send you to anybody. So I might have to have my patients travel a little bit, but once you've reached a point and you understand what you're going through and you've gotten to that like, I have to do something about it, it's never usually an issue. They want to see the correct person, or don't mind the travel.
Wardee: Sure. Of course. I found it very convenient to meet with you online every day. I would have been willing to go to somebody local, but I really wanted a virtual solution.
Melissa: And that's a blessing. Faceology is great for that. Yes, it's a blessing. I feel like after COVID, people were able to adapt. You think, oh, just younger people do all this. I had a patient I told you about just the other day. She's 80 years old that I worked with and did telehealth, and she did perfectly fine with it. So yeah, it is a blessing to be able to reach so many different people at so many different locations.
Wardee: Okay. Let's talk now about women our age. Although I know I'm like almost 10 years older than you, but I'll just say I'm your age. We are particularly affected by myofunctional dysfunction, and there's a lot of women our age who are going to be listening to this. So I want to particularly address this audience. So tell us what you know.
Melissa: So I have a lot of people that come to me... perimenopause, menopause, different kind of age ranges and groups in there... and talking about the OMDs. They might not have realized in the past that's what was going on, but there's always been some type of underlining issue there. But it seems to be, especially like after you have a baby or after you're going into menopause, like I said, when the hormone fluctuations start to happen... those little things were smoldering in the background, but you can't deny once it really lights a fire inside of you. There's things that start happening. You talked about your sleeplessness, and that's issues with airway. Going back to that, some of my patients come to me with TMD issues. That's things going on. So let me try to correlate both of those. So those are usually the main tickers. It's my jaw...
Wardee: Okay. And just, real quick, if you would say what OMD means... because I'm not sure we've defined that, and I can't recall.
Melissa: No, I'm so sorry. So OMD is orofacial myofunctional dysfunctions or disorder. Dysfunction.
Wardee: Okay, great.
Melissa: So it can, again, be the jaw pain, the obstructive sleep apnea, the different things that your body's doing and functioning, as it's causing issues. So I'll go back to the TMD, enrolling it into the sleeplessness, the UARS, which I'll define... that's upper airway resistance syndrome... and obstructive sleep apnea. Sometimes I say that as OSA.
So let's say you are middle age and your hormones decide to go haywire. We as women... everyone... we have estrogen receptors. There's a lot in our temporomandibular joint. There's a lot in our masticatory muscles. And when those fluctuations happen, that can cause issues with our joint fluidity, our cartilage integrity, and it can also increase pain perception in that area. Sometimes they wake up and they're like, oh, I'm clenching and grinding, or I'm just not sleeping well. There's a lot of stuff going on.
And of course, too, when hormones fluctuate, we end up losing some muscle tone. Not just here, I mean, in the body. So we get some instability here. We get some pain arousals there. You are not sleeping well. And if that low muscle tone, of course, starts rolling you into UARS, upper airway resistance syndrome, meaning you are not having a full-on obstructive collapse... if you are having that, an OSA, the obstructive sleep apnea... but it's enough where you're having arousals at night.
Now I'm going to jump around with this too. The arousals, especially in middle-aged women, it can be clenching and grinding, but it can also be getting up to have to use the potty. Did you have that? It's like, every time I go to sleep, within two or three hours I'm having to get up, or this or that or the other. When you have those arousals, when that desaturation happens, there's a jump inside that's happening. It goes basically back to your parasympathetic system, kind of fight and flight. Let's talk about chemically fight and flight. So when your body desaturates, it's going to try to arouse you to wake you up because it wants you to breathe. And again, it can clench your jaw, or it can cause you to feel like you have to urinate. That happens because this big adrenaline dump occurs.
Wardee: Yes.
Melissa: And when the adrenaline dump occurs, you have this contraction of the bladder. It doesn't mean to do that, it's just happening in the background. But that contraction happens and you get woken up and you have to go to the potty. It happens in kids, you see this a lot of times with the children, the chronic bedwetting. It goes back to airway. Pretty much every time.
When you are feeling that, or you didn't sleep, you're waking up with pain, you've been up all night... the next day, you're never catching up. You're not getting your rest and digest, you're never getting your regenerative, you feel better. So now you're getting the brain fog. Now you're getting chronic issues. UARS is actually pretty hard to diagnose. You have to find a really specifically trained sleep doctor, because it doesn't show up as OSA. You're not having these huge obstructions where you're desaturating. You're not even sometimes hearing UARS. Of course, if you have someone at home, your spouse, and they'd be like, you're snoring, or you're doing this, and you're like, okay, something's going on.
So I also want to say this... just because it's common doesn't mean it's normal. Snoring is very common, but it's not normal. It's not healthy. In kids and adults. So it's a big deal. And a lot of people are like, oh, that baby's laying there, and look at how big they're snoring. And I'm like, ah, it's a red flag automatically.
But as those things compound, you have all these things going on inside the body. I've had women that have come to me with being diagnosed with depression, with chronic fatigue syndrome, even fibromyalgia, and it all has gone back to being truly an airway issue that had just been not diagnosed correctly and not supported.
Wardee: Wow.
Melissa: It's a big deal. I never say sleep apnea is going to be the thing that takes you out, but it's a comorbidity of it for sure.
Wardee: Oh, absolutely. That's right.
Melissa: But yeah, hormones and fun, fun times. It all snowballs and works all together.
Wardee: Yeah. So I guess the point is it's like aggravation upon aggravation at this time of life, and maybe one of those things, we'd be doing okay. But because we have the hormone fluctuations, and then we have the pain, and then we have the arousals, and we're not getting our rest, and it's just snowballing into an untenable situation.
Melissa: Absolutely. Absolutely. And I'm not saying that myofunctional therapy cures all of it, it helps to get down to the root issue. Because if you can sleep better and you can breathe better, it sets you up for the next day better, and therefore... I think I've told you this before... we're like onions. We're layering. I've got to peel those layers back. I've got to get to that core. And you might cry along the way.
Once you can get those foundational pieces put into place... and a lot of the things that I'm working with, you don't have to do exercises forever. It's about awareness. And just like you said, you can't go out in public now without seeing it. You have such awareness of your body and everything else. It helps you to pick up on other things of what's going on with your body, which might lead you into adding the next layer that's going to be supportive on your journey. So it's peeling it back and then adding to it. It's just foundational stuff that we're working with.
Wardee: Yep. Okay. That is a perfect tee-up for my next question, which I'm going to start by sharing a little story with everybody who's listening. It's not a huge story, but when I first started working with you, Melissa, I was somewhat in a panic because I was sleeping so poorly. And I had already had my myofunctional assessment, saw what the dysfunction was that was going on. And Melissa Mogno, your... I'm not sure she's your clinical director.
Melissa: Clinical director.
Wardee: Okay. At Faceology, she was saying, yes, we can help you. And I already had my first appointment with you scheduled. Anyway, so I met with you for the very first time, I guess I was in that panic situation, but you talked me off the ledge because you talked to me about the layers of the onion. You also were like, I know you're not sleeping well, but we have things we can try. I'd like to work with you, and I'd like you to be giving me feedback so that we can develop this as we go, rather than jumping to... and you didn't tell me not to do that. You just said, if you would consider working with me, you might end up at a happier place. And let's just see where this goes. Can you be patient? And I basically said, yes, I can be patient. That really resonates with me.
So that's my little story to lead into my question for you, which is... what is your approach with people to help them when they are desperate for sleep? I know what you did with me. I don't know if you do that with everybody, but I'd just like you to talk through your process. What do you do first? What do you do second? What do you do third? And the goal being, you're going to fix it when somebody's messed up. So how do you fix it?
Melissa: There's a beauty of being telehealth because I can see and reach so many people, but I can't physically get in there and touch things like I can if you're in my clinic. So I try to get you in front of an airway knowledgeable dentist provider so they can look in and see, maybe if something's going on. I also like to work with a patient initially first, because I have different things and cues. I'm going to go back to this Myo Munchee right here. If I have you stick this in and I say, just hold it, hold it for two minutes, and I see little things like your nostrils start flaring, or your eyes get really big and dilated, or if I see like the panic start to rise or the chest like... or I see that lip seal come apart, I go, there's more going on in there. There might be something obstructing up here, so I might need to get you in front of an ENT even before I start trying to get different things put into place.
So I try to rule out... anatomically there might be something going on. Sometimes there's polyps in the nose. Sometimes there's such a deviated septum that they're not getting enough airway. Even if I got their lips closed, they're just not getting enough oxygenation through there. So I usually have people see different providers. I sometimes have patients even see a sleep doctor, so we can get a baseline information of how they are sleeping, how many disturbances are you having and whatnot. Technology's great. We have a lot of patients that have the watches and different things.
Wardee: Yep. The Oura rings and stuff.
Melissa: That gives information. So I like having patients that can give me kind of a, hey, this is how it's going, because it helps me know by numbers. I know how you're feeling, but this is actually showing up good too.
So it really depends on where they're at. I try to meet the patient where they're at on their journey, how much bandwidth they have to go into those extra layers. Some people don't have the time, the money, or the flexibility at that point, so I have to meet them there. Some people are like, nope, I'm going to start with a CPAP. Or some people, let's say they come to me because they have a CPAP and they're not able to use it. It's really, they're struggling with it. I'm here to support you with that. I will meet you where you're at. I will try my best. If your goal is to try to wean off of it, I will try my best to do that.
We have different appliances too that an airway dentist can provide. They can do some different things. A mandibular advancement device, let's say... your habits made your form very narrow or very retracted. I have a little bit of, my jaw is slightly recessed, but I have some patients that are very recessed and their airway's about a coffee stir, and there's nothing that I can anatomically change about that. I can't expand you, and I can't do anything else. Like, you're stuck that way. But if we could even get just a little bit of movement forward at night to get that support... that jaw moved a little is a lot in the body. So just that little bit of movement right there can get you better sleep.
So I meet them where they're at. I try to support them. I have the goals I want to do. I always tell everybody, I'm going to meet you at a hundred percent, but you've got to work with me. You've got to put in the time, and we have to keep an open conversation of where you're wanting to land.
So I don't know if that really answers it, but...
Wardee: Yeah, it did. And I think what it did is confirm for me one of the best parts of my experience working with you or myofunctional therapy, which is... I looked at doing things on my own and I couldn't do the exercises, or I couldn't do it right, and I didn't know where I was going wrong. Is, am I physically unable to do this, or am I not understanding the instructions? I don't know what to do. And so you helped me with that, because you could tell me, actually, you're not ready to do these other things first. Or you would say, why don't you try this? And then that little cue, I could do it.
So depending on the different things, I guess it was just that feedback from somebody who knew where we were going, because I didn't really know where we were going and I didn't know how to get there. And that's what I hear you saying that you're doing with everybody, because everybody you work with, you have a goal for them. They have goals, you've got to work on it. But just to have that feedback to get there from somebody who knows is so valuable. I don't know that I would be where I am right now if I hadn't had the benefit of you and your expertise. I have no doubt that it made this huge difference.
Melissa: I think of it as... and this is from Melissa Mogno, she has really good things to make things click in your brain... but you can go to the gym and you can work out, but if you have somebody that's a trainer that knows how to isolate that muscle group or show you, all right, you have this goal, but let's work on this and that goal... that's really what I am, and that's what I'm here to support.
And the same thing too. I show up to our training session, but if you haven't been doing your exercises and homework in the background, you might not get the full benefit of doing therapy. So it's not just I show up with my 100%, you've got to show up too. You have to want it. You have to do the things in the background.
And to give a little insight, because people are like, how much are you doing? What in the world? Yes, I only ask 10 minutes really a day. A day of active exercises. And when I say active, I have our patients in front of a mirror. And the reason I have that is number one, so they can catch their compensations. Like I said, if muscles are engaging or doing certain things that they don't need to do, the patient can catch it and correct it. But it's also giving feedback to the brain. We're working on this neuroplasticity to some effect. Because if you have this poor habit and I'm trying to correct it into a better habit, it takes time to integrate. But if you can see it, identify, and feed that information, especially with tactile cues and stuff that I work with, it helps to rewrinkle and integrate a little bit faster too.
So active exercises, 10 minutes a day of your time. If you're doing it twice a day, and then I see you every two to three weeks. It's not a lot that you're having to live with me. But yeah, you've got to do the homework in the background.
Wardee: That's right. I definitely found it very doable. All right, let's talk about our children, the younger generation, children and grandchildren. I'll just bring up what I said earlier about, it's hard to unsee what you know now. But maybe this is new for a lot of people listening. But I think we are suffering ourselves, but also as nurturers... we care for our families so deeply. We don't want our children and our grandchildren to have the dysfunction or the compensations that get them to the same point where we are, if we are struggling. So what should we be looking for?
Melissa: We'll go all the way back. I know I keep saying pacifier and thumb sucking. This would be... it's always in the mouth. There's something that the body's craving, and the child's putting something in there, which is not optimal. Remember, muscle beats out bone. So if you have a pacifier in and the tongue is low, you're sucking all the time, or the thumb is in, you're already creating a dysfunction in the form of how that child's growing. So the body's craving something. That's telling me the tongue is low, or the tongue is even restricted. There can be other issues.
I said bedwetting. The arousals, whenever the child's not sleeping well at night. Clenching and grinding, even in children. Definitely snoring, definitely mouth breathing at night. Picky eaters is one thing.
Wardee: Picky eaters? That's cool. Yeah.
Melissa: Picky eaters. So for instance, if the tongue is restricted or if the tongue is low posture, certain textures and how they're able to manipulate their food... they sometimes have issues. Have you ever had an issue where you got easily choked, if you're drinking or eating or anything like that? If that becomes chronic as well, there's a dysfunction. That tongue's not able to work properly. It can be a thrust, it can be a lateral outside thrust, but there's something going on where the airway feels like, you're going to choke me. And therefore every time that happens with that texture, they go, nope, I can't eat that anymore. Nope, I don't want that. So picky eaters can even show up that way, or if you see that they have that kind of getting choked easy and different things.
Venous pooling... so venous pooling is something my daughter had. That is, as we sleep, we have fluid and different things in our face, and our lymphatic system kind of moves around. But if we have any obstructions in this area here, and we're not getting enough oxygenation, you can have kind of that dark underlining area of the eyes. So I have kids that come to me that have that zombie appearance. They're just sunken in and dark, their mouth's open, they're like struggling. You can totally tell that they're just not optimal. I can picture it.
After I swear, only three or four sessions, these kids come back, and that's full... they have this brightness to their complexion, their eyes look like they've got this new lease on life.
I'll roll into ADHD. I have kids that get sent to me with... I say the zoomies... these kids are already being classified by their teachers of, they might need to be put on medication, we don't know what's going on. I'm not saying that ADHD doesn't exist, or that some children don't actually need that. But most of the kids that I work with, it's airway. It all goes back to them not sleeping and breathing and functioning well. There are studies now that we have found whenever they are having sleep apnea issues at such a young age, their prefrontal cortex is not developing to the rate in which it should. So it affects their learning. It affects how they're able to bring in information. Of course, if they're tired throughout the day, they're not going to be the best student.
So even that... those symptoms of the venous pooling, their mouth being wide open, their ADHD tendencies, different things like that, all go back to airway. That's a big deal right now. I work with a lot of kids that are coming to me, but I'm always amazed it doesn't take long. Kids... not that adults aren't moldable, but kids, man, they're resilient, and they bounce back so quickly if we can figure out what's going on and address it. And again, it's not just me. I'm just one little piece of the puzzle. It's ENTs, it's orthodontists, it's body work. There's so many different facets that we use and work as a community together. But it's just such a blessing to... I work, again, five to 80 year olds, to see where people come to me and where they can link at the end of the day.
Wardee: I love hearing about the 80-year-old woman because it just shows she's still got a fighting spirit. Yeah. She's like, I can get better. I love that.
Melissa: It's never too late.
Wardee: Oh, that's wonderful. Now what about babies? So you don't work with babies, you start at five. You don't do babies?
Melissa: I don't work with babies because I feel like babies need more hands-on, and telehealth-wise, I can't do that. But I have a cousin that's in the lactation department. I'm pushing her to get her IBCLC. I'm like, we have to have somebody local. Like, she never even knew that this was something. That's what's so sad too. I went to dental school. I became a hygienist. Lots of dentists graduate. They are not getting taught this. I feel like this is starting to emerge now, but there's been just this huge gap in how that correlates with the whole body. But even with babies... so I'm trying to get her IBCLC so she can do a little bit more diagnosing. But yes, I feel like babies need more hands-on. There's different things, body-work-wise, certain cues. So I don't do babies. If I can get your attention span for just a little bit, that's usually when I start with five and I go up.
Wardee: That's wonderful. This has been so great, Melissa. Thank you so much.
Melissa: I've really enjoyed... I've, of course, enjoyed having you as a patient, but thank you for giving me the opportunity to hopefully get some more education out and get some awareness and different things that people might look at and go, huh, I see that now, and that could be this issue. So I'm here if anybody needs me. I work with Faceology. I'm sure Wardee can tag that too. But myfaceology.com, through the link. It's not just me. Lots of therapists.
That's a beauty too of Faceology. I'm not working as a solo practitioner. I have a group that... let's say I have a really complicated case, they've worked with certain individuals that maybe I haven't worked with. So I have this really community that I can pick their brain and get support with. And so that's a key part of it. I don't feel alone. You have a lot of support as a patient coming in, because you have not just me, you have a variety of people that can give different insights as well.
But there's so many different outlets too. I don't want to just plug us. I always recommend, you can Google airway dentist near me, or if you want to work with somebody in person. Sometimes patients do better with being in person. It makes them a little bit more accountable. So just look for myofunctional therapist near me. If you're getting on a website for an airway dentist, see if they tag little things like myofunctional therapy or different things of that nature that kind of goes, hey, they do know what they're talking about. So yeah, there's so much out there. If you feel like you need support, feel free to reach out. Our website has a lot of information, but a quick Google search... yeah, it can get your feet in the door of somebody that could be there to support you on your journey.
Wardee: Wonderful. We will wrap this up now, so be sure to look for all the information that's included with this interview, because we'll have links to Melissa's website, myfaceology.com, and I know there's an assessment and there's some things there if there's articles that people can read. There is a lot of information. I just so appreciate you being here, Melissa, sharing all your expertise, and I know it's going to be a help to so many. So thank you, and God bless you.
Melissa: Thank you. I really appreciate it, Wardee. Have a good day.
Wardee: Thanks. Bye-bye, everyone. God bless you.
Sign up to receive email updates
Enter your name and email address below and I'll send you periodic updates about the podcast.
Why Tongue Posture Matters
You might not have ever thought about where your tongue should be resting. I certainly hadn’t before working with Melissa. But it turns out that tongue posture is foundational to how we breathe, sleep, and even how our faces develop from birth.
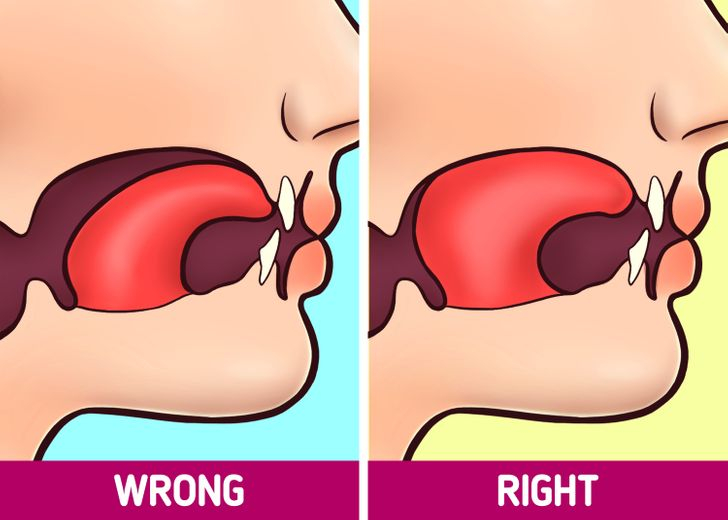
Melissa explains that when you’re at rest… not speaking, not eating… your tongue should be up in the roof of your mouth, lightly suctioned, filling into your palate. This matters because the tongue acts as the scaffolding of the upper palate.
When the tongue is in the correct position, it helps form the palate into a nice, wide U-shape. But the palate also serves as the floor of the sinuses. So when the tongue is where it should be, the sinuses develop more openly, and you’re set up for better breathing from the start.
When the tongue is low, though, the body starts compensating. Melissa shared her own experience as an example. She had a low tongue posture as a child, and her body craved something to fill that space… so she became a thumb sucker. That compensation shaped her into a specific phenotype: a narrower face, a deviated septum, chronic sinus issues. As she puts it, muscle beats out bone in the long run, and the tongue alone has 600 grams of pressure.
When the tongue is up and the lips are sealed, several important things happen. The airway is better supported at night. The soft palate is supported. And you breathe through your nose, which triggers your body to produce nitric oxide… a natural chemical that acts as a vasodilator, improves oxygenation, and is even antiviral and antibacterial once it enters the lungs.
God’s design really is perfect. As Melissa said, once you learn how the body functions and how integrated everything is, you have to acknowledge a perfect Designer. It doesn’t happen by accident.
What Is Myofunctional Therapy?
So what exactly is myofunctional therapy? Melissa describes it simply as physical therapy of the head and neck. You’re working on the face, the tongue, the lips, the throat… and of course, all of that connects back to the airway.
The foundational goals include correct tongue posture, lip seal, nasal breathing, and proper chewing and swallowing. But Melissa thinks of the body in terms of three pillars: structure and form, function, and habits. These three pillars interact with each other constantly.
Using herself as an example again: her low tongue posture (function) caused her palate to narrow (structure/form), which led to thumb sucking (habit). The cycle goes round and round. But the good news is that a myofunctional therapist can intervene at any point in that cycle.
Therapy involves exercises to correct habits, build awareness, and strengthen the right muscles. Melissa uses different modalities and appliances. For instance, a tool called a “myo munchie” that helps children (and adults) replace bad oral habits with better ones.
She also teaches patients to recognize their compensations. These are the ways the body adapts to dysfunction; things like forward head posture, using accessory muscles to breathe, jaw instability, clenching and grinding. Once patients can identify when those compensations are kicking in, they can start to correct them.
Tongue Ties: What They Really Are
Tongue ties are one of the most misunderstood issues in this space. Most people think a tongue tie means you can’t stick your tongue out. But Melissa explains that it’s really about how the tongue functions, not how it looks.
Everyone has a frenulum. That’s the tissue underneath your tongue. The question is how restricted that frenulum is. Tongue ties are graded on a scale of one through four. A grade one might not even be a true tie; it could simply be low muscle tone.
Which is exactly what happened with me. I was initially told I had a tongue tie, but after Melissa assessed me, she determined that I had some restriction but not to the degree that I needed a surgical release. My issue was more about low muscle tone, which we were able to address through therapy.
For a true tongue tie, the back or middle of the tongue is never able to fully reach up into the palate, even if the tip can get there. Melissa shared a fascinating detail: she’s worked with three speech language pathologists (SLPs) where two of them actually had tongue ties themselves, and one had low muscle tone. These are professionals whose job is to teach people how to speak and eat, and they didn’t even realize they had restrictions.
When the tongue is truly tied and can’t provide structural support to the palate, the form ends up narrower. Low muscle tone develops. Mouth breathing tends to take over, especially at night. And the body starts going through that snowball effect — airway issues lead to inflammation, which leads to more dysfunction, and on and on.
The Fascia Connection: From Tongue To Toes
One of the most fascinating things Melissa shared was about how the whole body is connected through fascia. This is a concept that’s getting a lot more attention lately.
There is a frontline fascia that goes from the tip of your tongue to the tip of your toes. Melissa thinks of the body in terms of “domes”: the upper palate, the esophagus, the diaphragm, the pelvic floor, all the way down to the arches of the feet. If something gets out of alignment in any of those areas, it can ascend or descend through the body.
She shared that when patients have a tongue tie release (done by a doctor with a laser), the effects can be felt throughout the entire body. Some patients report that their chest opened up. Their shoulders dropped. One patient didn’t even realize how tight their feet had been until the fascia was released and they suddenly relaxed.
This is also why myofunctional therapy often involves a whole team of practitioners. You might end up working with an orthodontist, an ENT, a dentist, and a bodyworker… whether that’s a pelvic floor therapist, a cranial sacral therapist, or another specialist. The body is one integrated system, and addressing it requires looking at the whole picture.
Why Women In Perimenopause And Menopause Are Especially Affected
This is the section I especially want women our age to pay attention to, because this is where so many of us are struggling and don’t know why.
Melissa sees a lot of patients in the perimenopause and menopause years. Many of them have had some underlying orofacial myofunctional dysfunction (OMD) smoldering in the background for years, yet it’s the hormone fluctuations that really set things on fire.
Here’s what’s happening: as women, we have estrogen receptors throughout our bodies, and there are a lot of them in the temporomandibular joint (TMJ) and in our masticatory muscles (the muscles we use to chew). When hormones fluctuate, it can affect joint fluidity, cartilage integrity, and pain perception in that area. Add to that the loss of muscle tone that comes with hormonal changes, and suddenly you’re waking up clenching and grinding, or you’re just not sleeping well.
If that low muscle tone starts contributing to upper airway resistance syndrome (UARS) or obstructive sleep apnea (OSA), you start having arousals at night. And sadly, those arousals don’t just wake you up.
Because when your body desaturates (loses oxygen), it triggers your fight-or-flight response. A big adrenaline dump occurs. And that adrenaline dump can cause an involuntary contraction of the bladder. So all those middle-of-the-night bathroom trips may not be a bladder problem at all, they could be an airway problem.
This same mechanism explains chronic bedwetting in children, too. It goes back to airway issues almost every time.
When you’re not getting restorative sleep night after night, the effects compound. Brain fog. Chronic fatigue. Inflammation. Melissa has had women come to her who were diagnosed with depression, chronic fatigue syndrome, even fibromyalgia… and it all went back to an undiagnosed airway issue.
As Melissa said, just because something is common doesn’t mean it’s normal. Snoring is very common, but it’s not normal or healthy, in kids or adults.
The good news? Myofunctional therapy can help get to the root issue. If you can sleep better and breathe better, it sets you up for the next day better. And then you can start peeling back the other layers for deepest healing.
How Melissa Approaches Treatment
I want to share a little bit about what it was actually like to work with Melissa, because I think it’ll help anyone who’s considering myofunctional therapy.
When I first started, I was in a panic and considering getting on a CPAP machine. I’d already had my myofunctional assessment and knew there were dysfunctions. But at our very first session, Melissa talked me off the ledge. She said, essentially: “I know you’re not sleeping well, but we have things we can try. Be patient. Let me work with you and you give me feedback so we can develop this as we go.” And she was right.
Melissa’s approach is to meet patients where they are. She starts by ruling out anatomical issues. She might have you hold a myo munchie in your mouth for two minutes and watch for signs like nostril flaring, eyes dilating, panic rising, or lip seal breaking. If she sees those red flags, she knows there might be something obstructing the airway that needs to be addressed by an ENT before therapy can really begin.
Sometime she has patients see other providers when necessary, such as an airway-knowledgeable dentist, or a sleep doctor for baseline data. She also uses technology like fitness rings and smartwatches for feedback. Numbers help her know what’s actually happening, not just how you feel. (Not all of this is needed, you can simply start by availing yourself of Melissa and go from there!)
Note: I, Wardee, wear the RingConn 2 (not Air) because you don’t need a subscription and it is extremely low EMF and has an airplane mode, too! If you prefer a watch, you might consider the Garmin Vivoactive 6, which is also low EMF and doesn’t require a subscription.
Some patients come to her already using a CPAP and struggling with it. She supports them there, too. Some patients may benefit from a mandibular advancement device from an airway dentist, because even a small amount of jaw movement forward at night can make a significant difference.
Note: You might consider using the Reviv 3 mouthguard as a mandibular advancement device (use code WARDEE to get 10% OFF). Ease into it, as it may be uncomfortable. Additionally, you might benefit from a custom device through an airway dentist if you have any trouble or persistent discomfort.
As for the actual therapy work, Melissa only asks for about 10 minutes of active exercises per day, done in front of a mirror. The mirror is important because it helps you catch compensations (muscles engaging that shouldn’t be) and it provides visual feedback to the brain. This helps with neuroplasticity and integrating the new, better habits faster. Sessions with Melissa happen every two to three weeks. It’s very doable.
I can personally say that the feedback from a trained therapist made all the difference for me. I tried doing exercises on my own first and couldn’t figure out if I was doing them wrong or if I was physically unable. However, Melissa could tell me, “You’re not ready for that yet… do this first.” Or she’d give me one small cue and suddenly I could do it. Having that expert guidance was invaluable and I know I made progress faster because of it. Plus, I could tell I was on the right track, instead of wondering if I was off course or not.
What To Watch For In Children
As parents and grandparents, we can really make a difference. If we can catch myofunctional issues early, children are incredibly resilient and bounce back quickly.
Here are the signs Melissa says to watch for:
Pacifier use, thumb sucking, or always having something in the mouth. The body is craving something that the tongue should be providing. This tells Melissa the tongue is likely low or possibly restricted. And remember… muscle beats out bone. A pacifier or thumb in the mouth while sucking is already creating dysfunction in how the child’s face and palate are growing.
Bedwetting. Just like in adults, chronic bedwetting in children often goes back to airway issues. The child’s body desaturates during sleep, triggers an adrenaline dump, and the bladder contracts. It’s not necessarily a behavioral issue; it could be a breathing issue.
Clenching and grinding, even in children. Yes, this happens in kids, too!
Snoring and mouth breathing at night. Snoring in a child is always a red flag. It’s common but never normal.
Picky eating. This one surprised me! If the tongue is restricted or has low muscle tone, certain textures become difficult to manage. The child may feel like they’re going to choke, and they start refusing those foods. It’s may not be stubbornness, it could be a functional issue.
Venous pooling (dark circles under the eyes). If a child has obstructions in the nasal area and isn’t getting enough oxygenation, you can see that dark, sunken appearance under the eyes, what Melissa calls the “zombie appearance.” After just three or four sessions, she sees these kids come back with brightness in their complexion and a new light in their eyes.
ADHD-like symptoms. This is a big one. Melissa works with many children who have been flagged by teachers as potentially needing medication. She’s not saying ADHD doesn’t exist, but most of the kids she works with turn out to have airway issues at the root. Studies now show that sleep apnea in young children can affect prefrontal cortex development, which impacts learning and the ability to take in information. A child who isn’t sleeping well is not going to be the best student.
Melissa’s Story: From Hygienist To Myofunctional Therapist
Melissa’s path to myofunctional therapy is a beautiful story of God’s guidance through closed doors and opened windows.
She had been a dental hygienist for 20 years when her daughter became the catalyst. In 2018, when her daughter was five, she had already had ear tubes placed twice, a sinuplasty, and adenoids removed. Melissa’s daughter was a textbook obstructive sleep apnea case, but living in South Georgia meant limited access to airway-knowledgeable practitioners.
Melissa discovered myofunctional therapy and knew immediately it was what she needed to learn. But life kept intervening: her husband’s job demands, her daughter’s sports schedule, then COVID in 2020. Then the boss she’d worked with for 15 years was unexpectedly diagnosed with cancer and passed away within two weeks.
Through all of it, the Lord kept bringing her back to this calling. Eventually she connected with Sarah Hornsby and learned about Faceology. She took a chance and reached out, asking if there was a need for a therapist in South Georgia. The answer was yes, and especially because Melissa’s Eastern time zone was ideal for working with patients across Europe via telehealth.
Today she works with patients from age five to eighty, across the U.S. and internationally. She has the support of a whole community of therapists at Faceology, which means even complicated cases benefit from multiple perspectives. It’s never just one practitioner working alone.
Where To Go From Here
If you’d like to work with Melissa or another myofunctional therapist through Faceology, visit myfaceology.com. The website has a wealth of information, and you can find an assessment to see if the therapy would be right for your situation. Telehealth makes it accessible no matter where you live.
If you’d prefer to work with someone in person, Melissa recommends doing a quick search for “myofunctional therapist near me” or “airway dentist near me.” When you’re looking at an airway dentist’s website, check whether they mention myofunctional therapy… that’s a good sign they understand the bigger picture.
It’s never too late to start. Melissa works with patients from age five all the way to eighty years old, and she has seen transformation at every age. Kids bounce back remarkably fast, but adults can make significant progress, too.
As Melissa reminded us, we’re like onions. It’s about peeling back the layers, getting to the core, and then building a strong foundation. Once those foundational pieces are in place, you don’t have to do exercises forever. It’s about awareness. And once you have that awareness… you really can’t unsee it!
God bless you on your journey to better health!
Helpful Links
- myfaceology.com
- Reviv 3 Mouthguard (clenching, grinding, mandibular advancement) — use code WARDEE for 10% OFF
- RingConn 2 (not Air)
- Garmin Vivoactive 6 Watch
We only recommend products and services we wholeheartedly endorse. This post may contain special links through which we earn a small commission if you make a purchase (though your price is the same).

Leave a Reply